Evaluation of Skeletal Trauma
Susan L. Summerton, M.D.

Skeletal trauma: Goals
•Appropriate imaging evaluation
•What to look for
•What to order
•Pediatric skeletal trauma
•Child abuse
What not to order…..
•Just because we “can” image doesn’t meanwe “should” image…
•Consider $$, radiation
•Wastes patient’s, tech’s and radiologist’s time
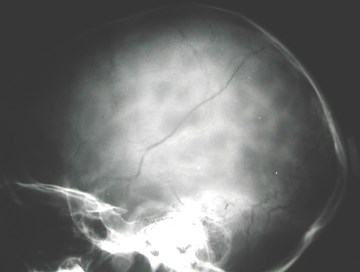
Unnecessary examinations: Skull Films
•< 10% of patients with fractures have subduralor epidural hematoma
•No findings on skull film indicate (or discount)subdural or epidural hematomas
•~ 60% with hematomashave no fractures
•Brain matters, not bones
Also…
•Coccyx
•Difficult to dx, not treated
•High radiation dose to gonadalarea
•Nasal bones
•Management depends onclinical findings


23 yo woman, “slipped on ice,fell on butt”
….and finally: Lumbar Spine
•Most abused exam in radiology
•No diagnostic info that will be acted on by a physician
•Greatest gonadal radiation dose of any plain film
•3 view lumbar spine has gonadal dose > 6 YEARSof daily chest x-rays.
•When to order:
•Severe trauma
•Possible primary or metastatic tumor
•Possible infection

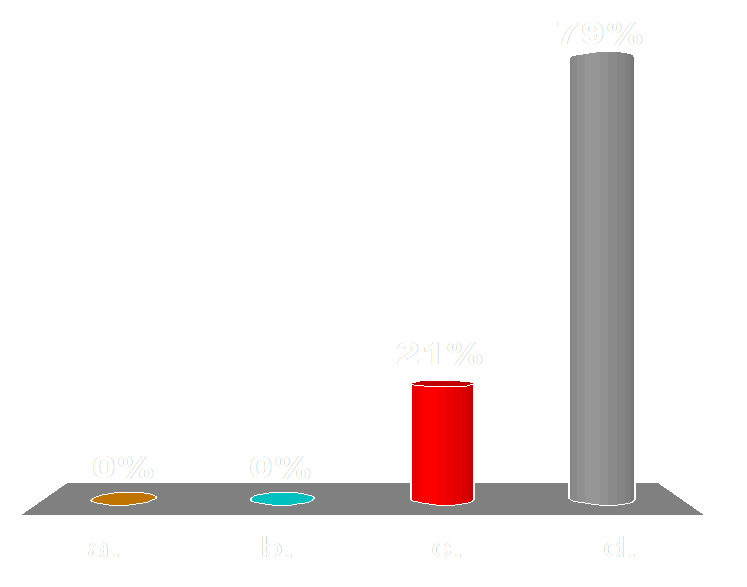
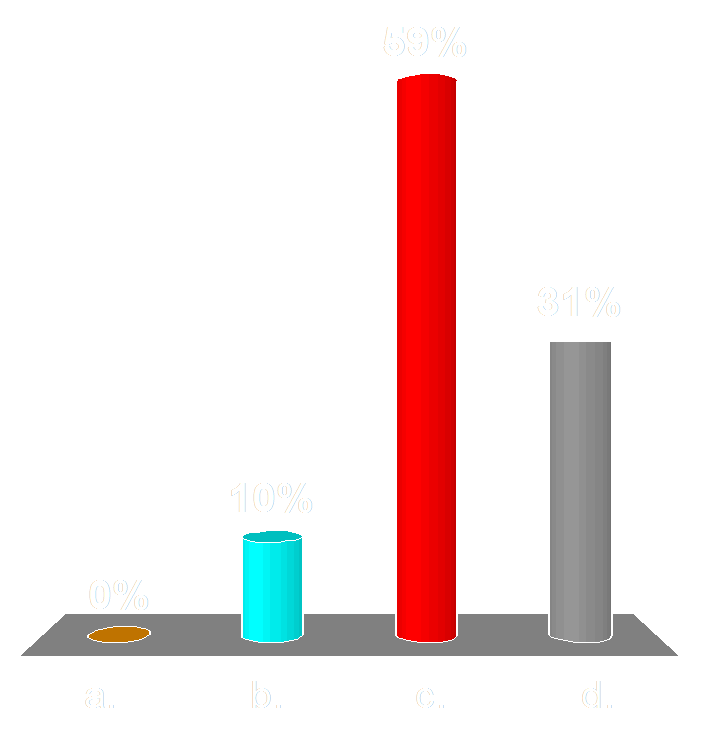
A 15 yo boy twisted his knee. X-rays are normal, but hissymptoms are still severe. The most appropriate next imagingstudy is…
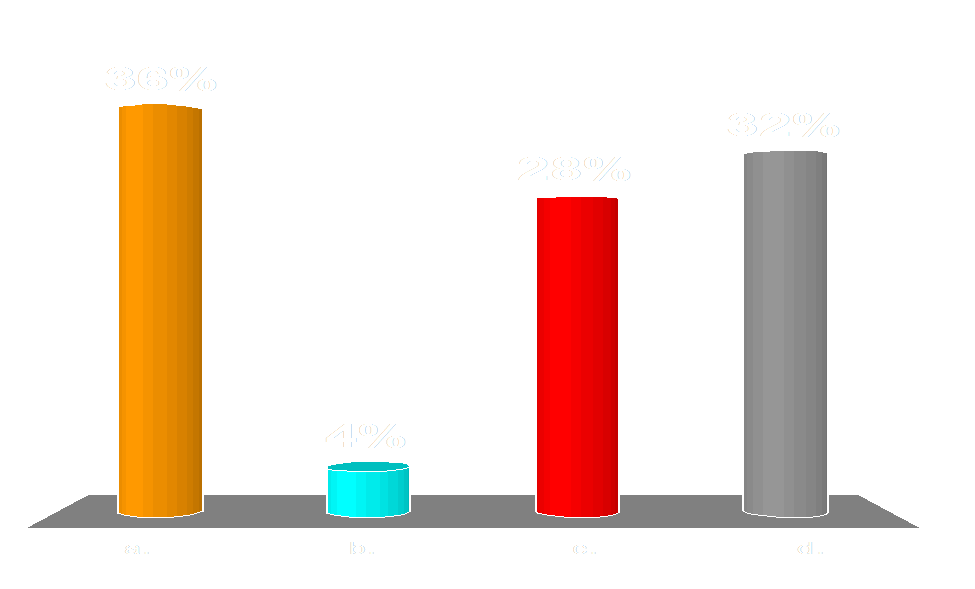
Audience Question
a. CT scan
b.Bone scan
c.MRI with contrast
d.MRI without contrast


Imaging Modalities
•Radiography 1st - bones, joints (soft tissues)
•MRI - good for bones, joints and soft tissues
•Useful to detect occult fractures
•CT – helpful in surgical planning
•Not useful to detect occult fractures
•Bone Scan (scintigraphy) - for overall evaluation of allof the skeleton, particularly good for bone metastases
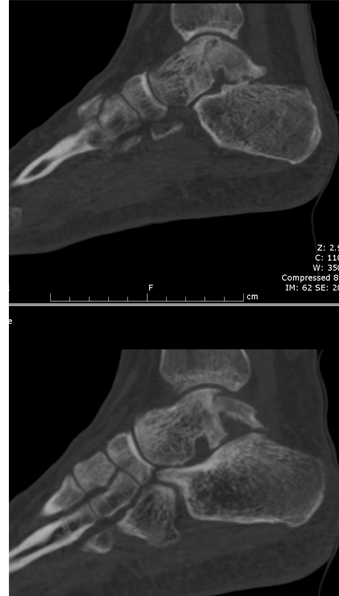
40 yo with persistent ankle pain twoweeks after he jumped off a fence.





Imaging principles in trauma:Rule of 2’s
•2 views: AP and lateral (1 view is no view)
•2 joints: include the joints above and belowfracture
•2 sides: both limbs
•Only if needed (in children with open epiphyses)
•2 occasions: Some non-displaced fractureswill not be visible for 10-14 days



2 views
30 yo male who twisted ankle







9 yo stubbed great toe, now it is swollen and shehas point tenderness over dorsum of IP joint



2 JOINTS


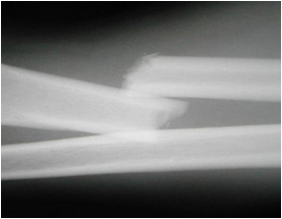
Another rule of 2’s:2 bones in extremity act as a ring
•Monteggia
•Ulnar fracture & radius dislocation
•Galeazzi
•Radius fracture & ulna dislocation
MUGR (mugger)
MonteggiaUlnar fracture
GaleazziRadius fracture

Radius
Ulna
Other areas that act as a ring
•Mandible
•Lower leg
•Pelvis




2 sides


RIGHT ELBOW: comparisonLEFT ELBOW: pain




December 9


December 23
2 occasions
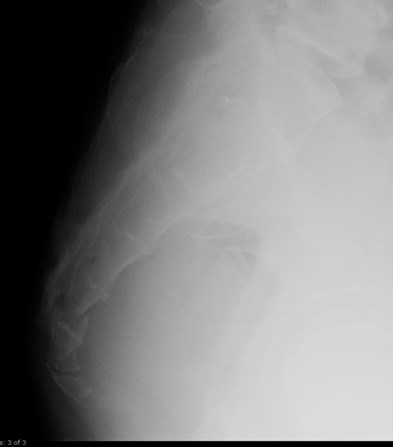
40 yo with shoulder pain following fall; is there afracture?
Audience Question

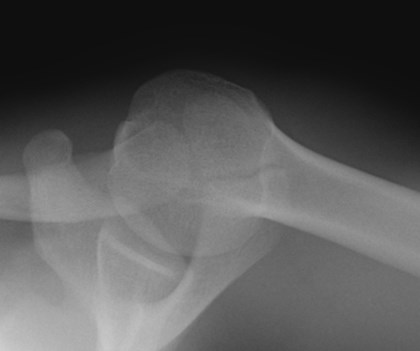
a.No
b.Yes
c.Maybe, I can’t tell, I need more views
d.No, but there is a normal anatomic variant that mimics a fracture
One important additional rule of 2’s
•2 radiographs
•Compare a difficult filmwith known normal film
•Compare to films inbooks that show normalvariants that may mimicpathology
Os Acromiale


40 yo with shoulder painfollowing fall
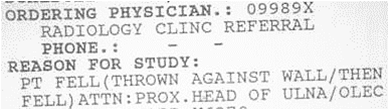
Having the proper history is crucial sothat the correct body part is imaged!
Study: Left Tib/Fib
History: Hit by parked car
Study: Left Shoulder
History: Fell on by heavier person
Study: cerebral angiogram
Reason: R/O subarachnoid hemorrhoids
Study: Testicular Ultrasound
Reason: R/O Oreochitis
Study: Left Shoulder
Reason: PT LEANED AGAINST MAN STANDINGNEXT TO HER WHILE BUS WAS MOVING.
Fracture Description:Definitions
Fracture: Complete disruption in the continuity of a bone
Dislocation: Complete disruption of a joint, articular surfacesare no longer in contact
Subluxation: Minor disruption of a joint, some articularcontact remains


Fracture types:Incomplete or Complete
•Complete
•Goes through entire cortex
•Incomplete
•Involves a portion of cortex
•Children
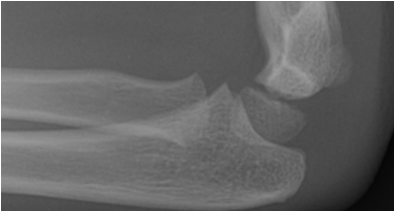
•Torus - buckle of cortex on compressive side
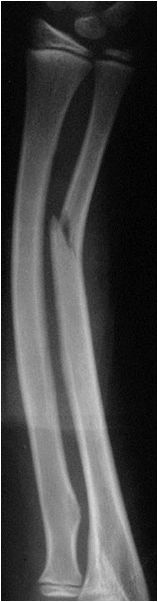
•Greenstick - fracture on tension (convex) side
•Plastic - bending without angular deformity andwithout subsequent remodeling


Buckle/Torusfracture
GreenstickFracture
Plasticfracture



Fractures in children:Salter Harris classification
•Epiphyseal growth plate involved
•alone or in combination with adjacent part of bone
•Why is this classification important?
•Has prognostic value
•Type I and II
–Do well
•Type IV and V
–Can develop early fusion of epiphysis
–Result in shortening of the limb
Salter-Harris I
•Fracture thru epiphyseal plate alone
•May be difficult to diagnose withoutcomparison of opposite side
•Must reduce if significantly displaced
•Require immobilizing cast
•Typically no growth disturbances
M
E

Salter-Harris II
•Most common type
•Fracture through growth plateand metaphysis
•“Corner Sign”-smallmetaphyseal fracture

Salter-Harris III
•Fracture through epiphyseal plate & epiphysis
•Rare
•Surgery sometimes necessary to restorejoint surface to normal
•Prognosis for growth is good if blood supply toseparated portion of epiphysis intact and iffracture not displaced

Salter-Harris IV
•Fracture throughepiphysis, growth plate,and metaphysis
•Surgery needed torestore joint surface andto align growth plate
•Prognosis for growth poorif surgery unsuccessful

Salter-Harris V
•Crush injury, growth plate compressed
•Uncommon injury
•Most occur at knee or ankle
•Prognosis poor for normal bone growth


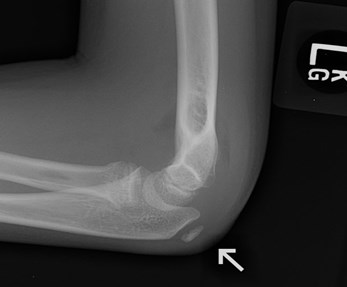
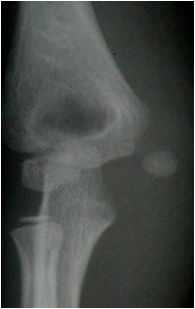
9 yo boy, pain following fall. This radiographshows:
Audience Question
a.Normal ossification centers in 9 yo
b.Horizontal fracture: proximal radius
c.Avulsion of capitellum
d.Dislocation of medial epicondyle
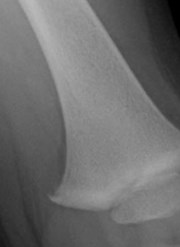
Analysis of pediatricelbow radiographs
•In kids
•anterior humeral line
•radiocapitellar line
•evaluate proper positionof ossification centers

Anterior humeral line
•Along anterior humeralshaft on lateral view
•Normally-Line passes thrumid 1/3 of capitellum
•Supracondylar fracture - anteriorhumeral line passes thru anterior1/3 or entirely posterior tocapitellum
humerus
ulna
radius

Radiocapitellar line
•Bisect proximal radial shaft, extend lineposteriorly
•Normally - line passes thru capitellumon all views
•If not, radial head dislocation or capitellumdisplacement should be suspected
ulna
humerus
radius

MedialEpicondyle

Medial epicondylar ossificationcenter injuries
•Most common ossificationcenter involved by trauma
•Frequently isolated injury
•+/- elbow dislocation
•Look for medial epicondyleossification center in everypediatric elbow case

Surgery indicated when:
1) medial epicondyle ossification center displaced > 1 cm
2) when ossification center incarcerated within elbow joint
Elbow ossification centersCRITOE
C
R
E
I
T
O
•Capitellum1 year
•Radial head5 years
•Internal (medial) epicondyle7 years
•Trochlea10 years
•Olecranon10 years
•External (lateral) epicondyle11 years
•Get comparison views of opposite side if unsure


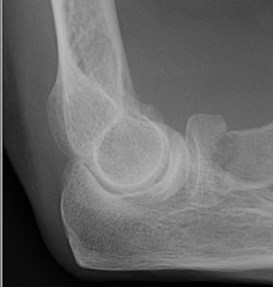
3 yo with elbow pain following FOOSH
C
R
E
I
T
O
•Capitellum1 year
•Radial head5 years
•Internal (medial) epicondyle7 years
•Trochlea10 years
•Olecranon10 years
•External (lateral) epicondyle11 years

Child Abuse
•3rd most common cause of childhood death
•(SIDS, accidents)
•20-40% of abused children have skeletal trauma
•Most common sites long bones, skull
•Consider child abuse when…
•unexplained injury
•fracture appearance discordant with proposedmechanism of injury
Child Abuse:Highly specific fractures
•metaphyseal fractures
•posterior rib fractures
•scapular fractures
•spinous process fractures
•sternal fractures
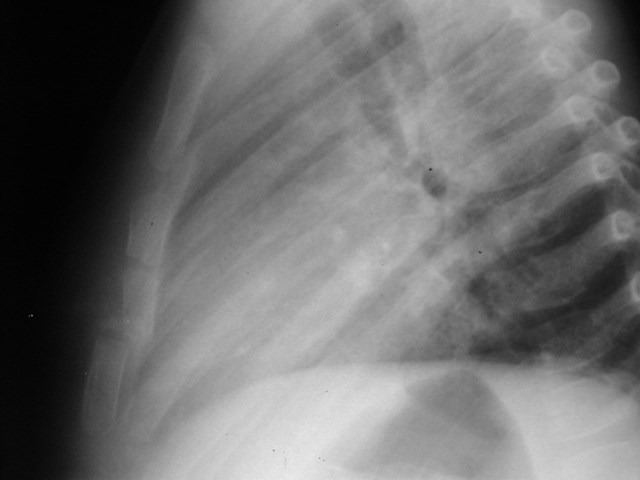
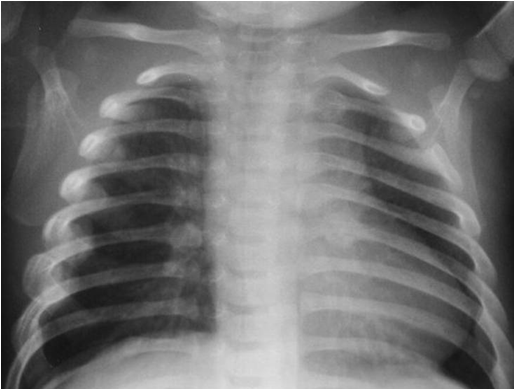
Sternal fracture
Rib fractures
•Rare in accidentaltrauma due toplasticity of ribs
•Posterior fractures
•Costovertebraljunction
Moderate specificity
•multiple fractures (especially if bilateral)
•fractures of different ages
•epiphyseal separations
•vertebral body fractures
•digital fractures
•complex skull fractures
Common but low-specificityfractures in child abuse
•clavicle fractures
•long-bone shaft fractures
•linear skull fractures
Moderate- and low-specificity fracturesbecome highly specific when a crediblehistory of accidental trauma is absent,particularly in infants.


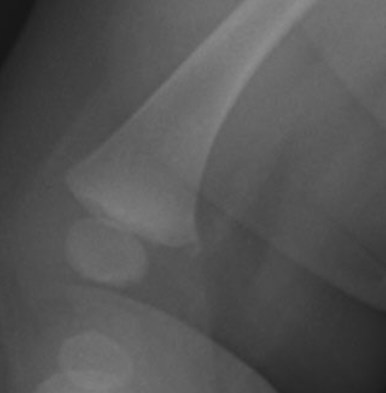
Pathognomonic Signs
•Fractures at different sites anddifferent stages of healing
•Metaphyseal fractures
•Due to traction on limb
•Uncommon with accidentaltrauma < 5 yo


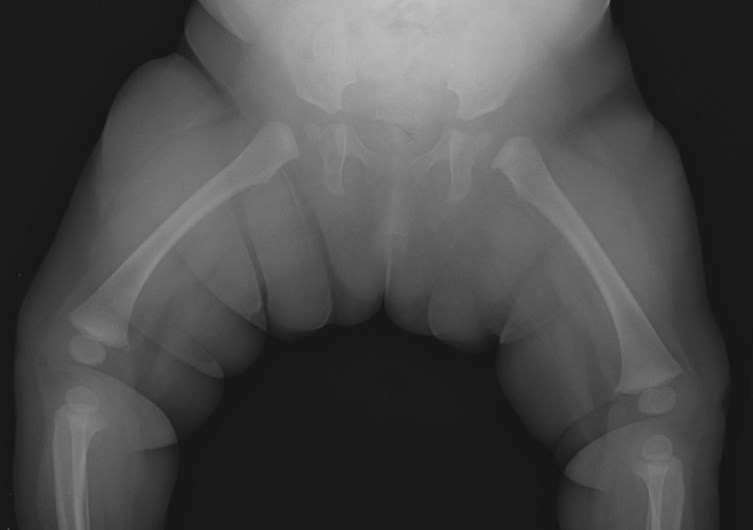
Metaphyseal corner fracture